
Good clinical practice starts with good clinical documentation. How can you know how well you are doing for your patients if you don’t document what you are doing and the results of your care.
During a recent webinar entitled “Legal Perils and Pitfalls of Wound Care” Heidi Cross provided some useful tips on documentation. Here are the top ten tips regarding good documentation practice and some do’s and don’ts.
1. VISUAL INSPECTION

Start by looking and describing what you see. It’s important to make consistent, accurate notes on both the patient and their skin (and or wound).
 DO | Describe what you see |
DON'T | Guess at the type or the stage of a pressure injury or the depth of the wound, or stage a wound a certain way just because that is what the last shift documented. |
2. PRESSURE INJURY RISK ASSESSMENT

When specifically looking at the risk of pressure injury, ensure a full skin and patient assessment. Know which scoring system is used and ensure the correct score is recorded for your patient.
| DO | Perform a pressure injury risk assessment and know correct subscores. |
DON'T | Rely on previous risk assessment scores. |
3. PRECISE USE OF LANGUAGE
Clear communication is important. A critical component of good communication is language. Language is important on so many fronts both with respect to your continued understanding and assessment of the patient with time; to communicating with others in the care team and sadly, if required, in a court of law to justify your actions.
| DO | Be very specific in your note about any of your communications with other health care providers, the patient, or the family. |
DON'T | Generalize with statements like "Physician aware." |
4. PERTINENT INFORMATION TO INCLUDE

Ensure the pertinent information is recorded in your documentation. This is important for understanding or care given and resultant outcome. As is often stated “a picture paints a thousand words” so photography is a key component of pertinent information. But it not the only record and information required. Be as complete and descriptive as you can.
| DO | Record pertinent information in your wound care note, including dressing changes. |
DON'T | Just document "Dressing changed" or "Dressing dry and intact" in your note. |
5. WOUND CATEGORY CHANGES
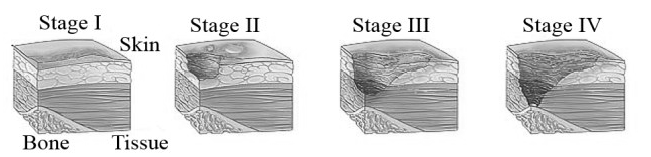
Pressure injuries should be recorded and staged. It’s a requirement of clinical practice. Staging and re-staging with time is vital to demonstrate changes in wound status. Also be careful not to miscategorise other wounds as pressure injuries as it has real, significant consequences. Especially with reporting.
| DO | Stage only pressure injuries and document when a wound changes category. |
DON'T | Document a skin tear, moisture-associated skin damage, a venous ulcer, an arterial ulcer, or a wound with any other etiology as a pressure injury. |
6. PATIENT BEHAVIORS
If any patient behaviour has an impact on your ability to deliver care it is important that you document what and why? Try not to judge but rather document the facts as they occur. We all know what its like to be a patient so have some empathy to why their behaviour is what it is.
| DO | Describe in the medical record behaviors of patients that complicate care. |
DON'T | Be judgmental, using terms that imply judgement. |
7. REFUSAL OF TREATMENT

As with each and everyone of us we have the absolute right to refuse any aspect of our care. Patients therefore have that right. It is important to record this and to record it accurately and how you think it will impact their care. More importantly record any education or corrective actions you may have taken to influence the patients decision.
| DO | Describe in the medical record the who, what, where, why, and when of refusals of a treatment or care. |
DON'T | Forget to chart what actions you took and what education you provided, as well as the patient’s reaction. |
8. HIPAA-APPROPRIATE PHOTOGRAPHY

Quality, safety and privacy is vitally important when handling patient information. This is especially true when handling photographs. There are rules and regulations provided by HIPAA to protect patients and it is important that such regulations are adhered to in each and every case.
| DO | Follow your facility guideline regarding photography. |
DON'T | Cut corners when it comes to photographs. |
9. END-OF-LIFE WOUNDS

End of life is a special circumstance and requires significant empathy. It is important to identify such wounds and to ensure appropriate care is provided. Of more importance is the documentation of the end-of-life status. These are special circumstances and skin failure is inevitable and a consequence of the process.
| DO | Distinguish end-of-life wounds from pressure injuries or other wounds. |
DON'T | Overlook skin failure at end of life as a causative factor in skin breakdown. |
10. UNAVOIDABLE PRESSURE INJURIES

Unavoidable pressure injuries are a fact of life. More importantly they need to be recognized and documented. CMS recognizes unavoidable pressure injuries but requires early recognition and also the assurance that best practices were implemented to provide optimal care, both early in the diagnosis but more importantly ongoing.
| DO | Document in the medical record the circumstances and risk factors that make a pressure injury "unavoidable". |
DON'T | Avoid addressing the issue of "unavoidability" in the medical record if it is relevant to an individual patient's wound. |




